Branding as the Foundation of Effective Plastic Surgery Marketing
From Eminence: The New Standard of Plastic Surgery MarketingStrong branding is associated with greater demand, premium pricing, greater resilience during market shifts, and stronger long-term financial performance.
The Unintentional Brand
Most surgeons, if asked whether they have invested in branding, would say no, or would describe having a graphic designer assist them with a logo and a web designer with a website, and leave it at that. Branding carries associations that feel incompatible with medical culture: the management of image over substance, facade over outcome. This is a reasonable instinct in a field where professional reputation is built over years of clinical practice. The problem is that emotional responses can shape whether patients continue evaluating a practice after landing on a website or seeing its social content.
While branding has been extensively studied in consumer goods and mainstream service industries, research in healthcare and medical-aesthetic services has emerged more recently. Bank and colleagues provide one of the few empirical accounts linking branding to measurable performance outcomes in plastic surgery. In their case study of a New York-based plastic surgery group practice, the authors documented the process of rebranding through a new website, unified visual identity, and coordinated social media marketing. Following implementation, the practice reported a 91% increase in website traffic, an 82% rise in website sessions, and a 21% growth in new patient volume.
A brand forms whether it is intentionally designed or left to chance. Every patient-facing element from before-and-after photography to website copywriting, review responses, and the physical experience of the consultation room, contributes to the practice’s brand perception. Designing a brand intentionally creates the opportunity to present the practice as it wants to be perceived. Leaving it to form on its own produces whatever impression the available materials happen to create, which is rarely the most accurate or compelling version of what the practice actually offers.
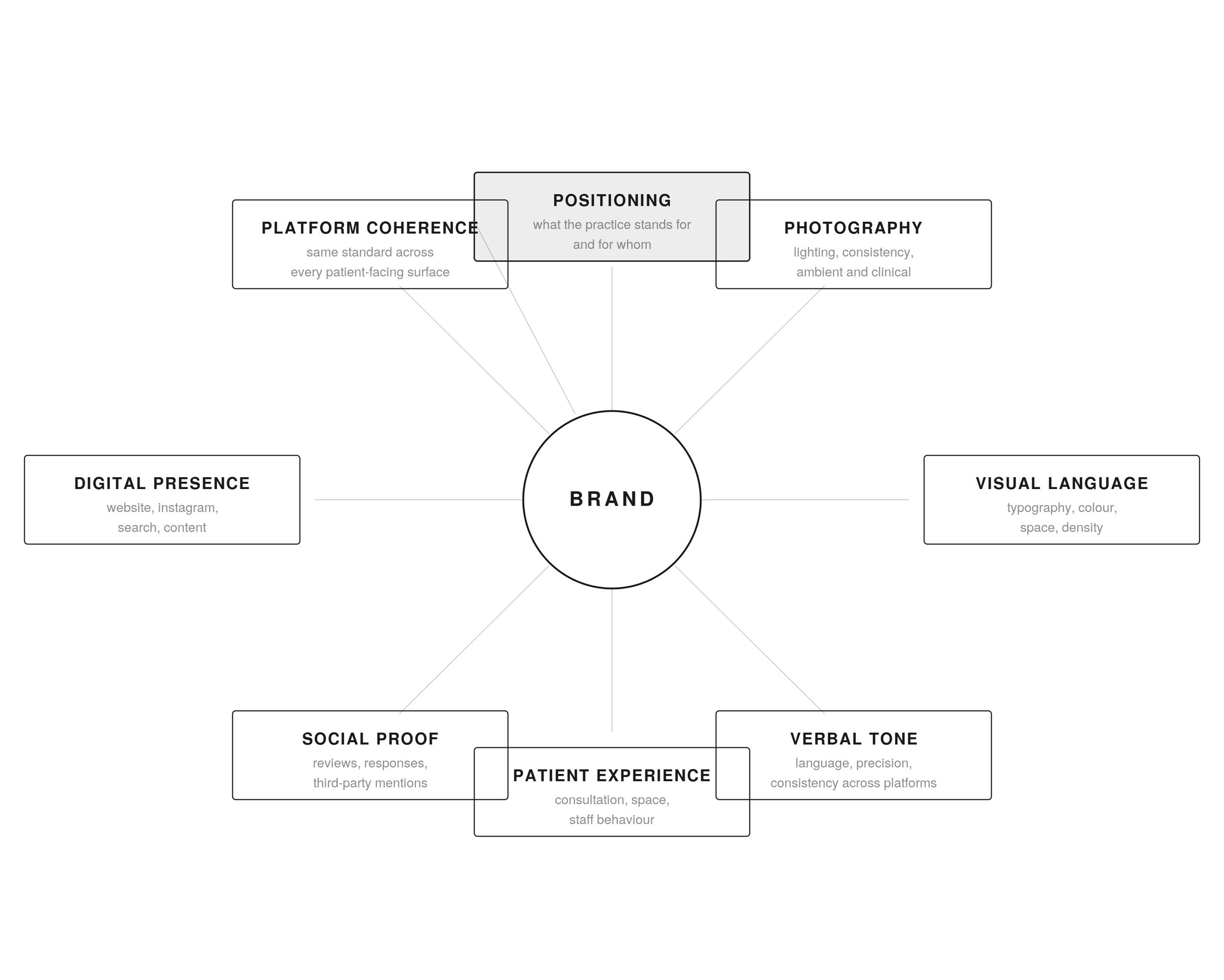
A brand forms whether it is built intentionally or left to chance. Every patient-facing touchpoint, from positioning and photography to language, reviews, digital presence, and the patient experience with clinic staff, contributes to how the practice is perceived.
Patients Choose With Emotion and Justify With Logic
The business case for branding begins with how high-stakes decisions are actually made. People often believe they reason their way to a conclusion, but high-stakes decisions are often shaped by emotional responses, then evaluated through rational criteria.
One of the most widely accepted ideas in cognitive psychology is that human judgment operates through two modes of thinking. Psychologist Daniel Kahneman won a noble prize because his research proved that human beings are not entirely rational and rely on intuitive shortcuts, heuristics, and cognitive biases that often lead to irrational decisions.
According to Kahneman, most of our thinking is fast, automatic, intuitive, and emotionally guided. He calls this System 1 thinking. System 2, on the contrary, is deliberate and analytical. Branding influences the initial reaction of System 1. If the practice feels trustworthy, refined, and consistent, the patient is more likely to keep paying attention and review the surgeon’s work more closely. If the first impression feels unclear or inconsistent, the patient may leave before carefully evaluating the surgeon’s work and experience.
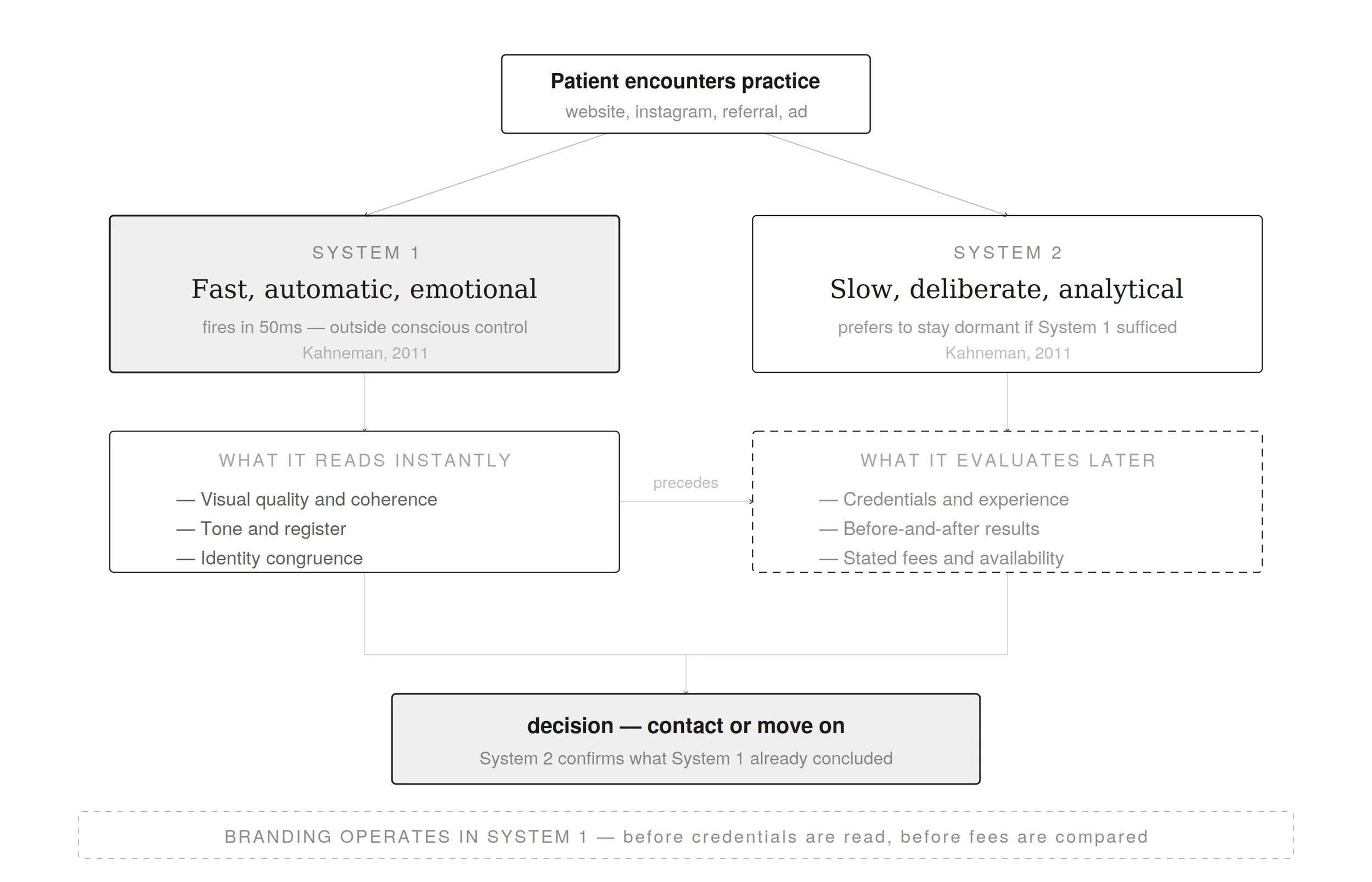
The dual thinking process and branding. Branding shapes the first impression before rational comparison begins. Patients may later evaluate credentials, fees, and results, but the initial sense of trust, quality, and fit is formed almost instantly through visual and emotional cues.
Emotion helps the mind assign weight to information. The neurologist Antonio Damasio documented this through clinical observation of patients with damage to a certain brain region involved in emotional processing. These patients retained reasoning, working memory, and language comprehension, yet struggled to make everyday decisions. Damasio’s hypothesis proposed that emotional responses function as essential inputs to decision-making. Without the ability to assign emotional weight to options, the brain struggles to resolve complex choices, even when the factual information is complete. Although direct evidence from plastic surgery remains limited, the same decision-making mechanisms likely apply when patients compare surgeons and evaluate treatment options. When qualifications appear comparable, patients often rely on how each practice makes them feel. This is a rational way to navigate uncertainty.
Branding Turns Marketing Spend Into Long-Term Equity
A practice spending several thousand dollars a month on paid advertising without a defined brand identity is distributing an unclear impression at scale. With a defined brand foundation, the same spend carries more value because each impression reinforces a specific market position and reason to inquire.
Branding may improve the impact of marketing spend by directing paid attention toward a coherent patient experience. Patients feel more assured about the quality of the practice when all patient-facing materials reinforce the same practice identity. This matters because marketing does not end when someone clicks an ad; the click only begins the evaluation process. A prospective patient still has to decide whether the practice feels worth contacting. Branding helps the patient understand what the practice stands for and what kind of expertise to expect.
Brand strength also influences commercial performance. Strong branding is associated with greater demand, premium pricing, greater resilience during market shifts, and stronger long-term financial performance. In a small exploratory perception study conducted by the author, forty participants evaluated branded and unbranded practice presentations. The results should not be treated as conclusive, but they support a pattern consistent with broader brand-equity research: coherent presentation can influence perceived trust, professionalism, and safety, and increase the intention to book and willingness to pay a price premium.
In the study, the participants that were shown two sets of practices with comparable credentials and results were more likely to indicate willingness to pay higher fees for the branded option. On a five-point scale, branded clinics scored 3.1 against 2.3 for their unbranded equivalents on willingness to pay a price premium, the largest gap recorded across the five constructs measured. Across the other four constructs, trust, professionalism, intent to book, and safety, branded clinics scored consistently higher in every category. The trust gap of 3.5 versus 2.8 and the willingness to pay a price premium gap emerged as the two most pronounced findings.
The qualitative phase of the study provided the reasoning behind these numbers. Many participants associated a coherent visual presentation with medical competence. Several equated good taste in digital presentation with good taste in surgical outcomes. One participant interpreted a modern visual identity as evidence that the surgeon stays current with developments in the field. The absence of a surgeon’s photograph, inconsistent design, and limited access to before-and-after imagery produced the opposite response: uncertainty, reduced safety perception, and lower intent to book.

Patient perception of branded versus unbranded practices. In a comparative perception survey of forty participants, branded clinics scored consistently higher than unbranded clinics across all five measured constructs. The largest gaps appeared in trust (3.5 vs. 2.8) and willingness to pay a price premium (3.1 vs. 2.3). On the willingness to pay a price premium construct specifically, 36.7 percent of branded-clinic responses fell at 4 or 5 on the scale, compared to 15 percent for unbranded clinics. The comparison was designed to isolate branding as much as possible across clinic presentations.
Plastic surgery marketing has become increasingly consumer-facing over recent decades, and many of the marketing standards are still forming. The research on how branding shapes consumer judgment is not new, but its application to aesthetic surgery is. Many practices currently look interchangeable online, even when their surgical work, patient experience, and professional standards are meaningfully different. That gap creates an advantage for the practices that choose to include branding as part of their marketing strategy before it becomes an industry standard.
Brand Positioning: Owning a Distinct Place in the Patient’s Mind
Before a practice decides how its website should look, what its social media should say, or how its advertising should be structured, it has to decide what position it should occupy in the market and in the patient’s mind.
Brand positioning distinguishes a practice from its competitors. In plastic surgery, this might mean the surgeon known for revision rhinoplasty, the practice focused on natural-looking mommy makeovers, or the clinic designed for international patients who expect privacy, coordination, and hotel-level service. When a practice is not known for anything specific, patients may fall back on secondary factors: price, proximity, availability, speed of response, or a friend’s recommendation. Those factors can weaken the advantage of a practice trying to build a premium, referral-driven business. A valuable position has three qualities: it must be distinct from what competitors already occupy, supported by the practice’s actual experience, and relevant to the patient that the practice seeks to attract. The illustration below displays the overlap of these qualities.
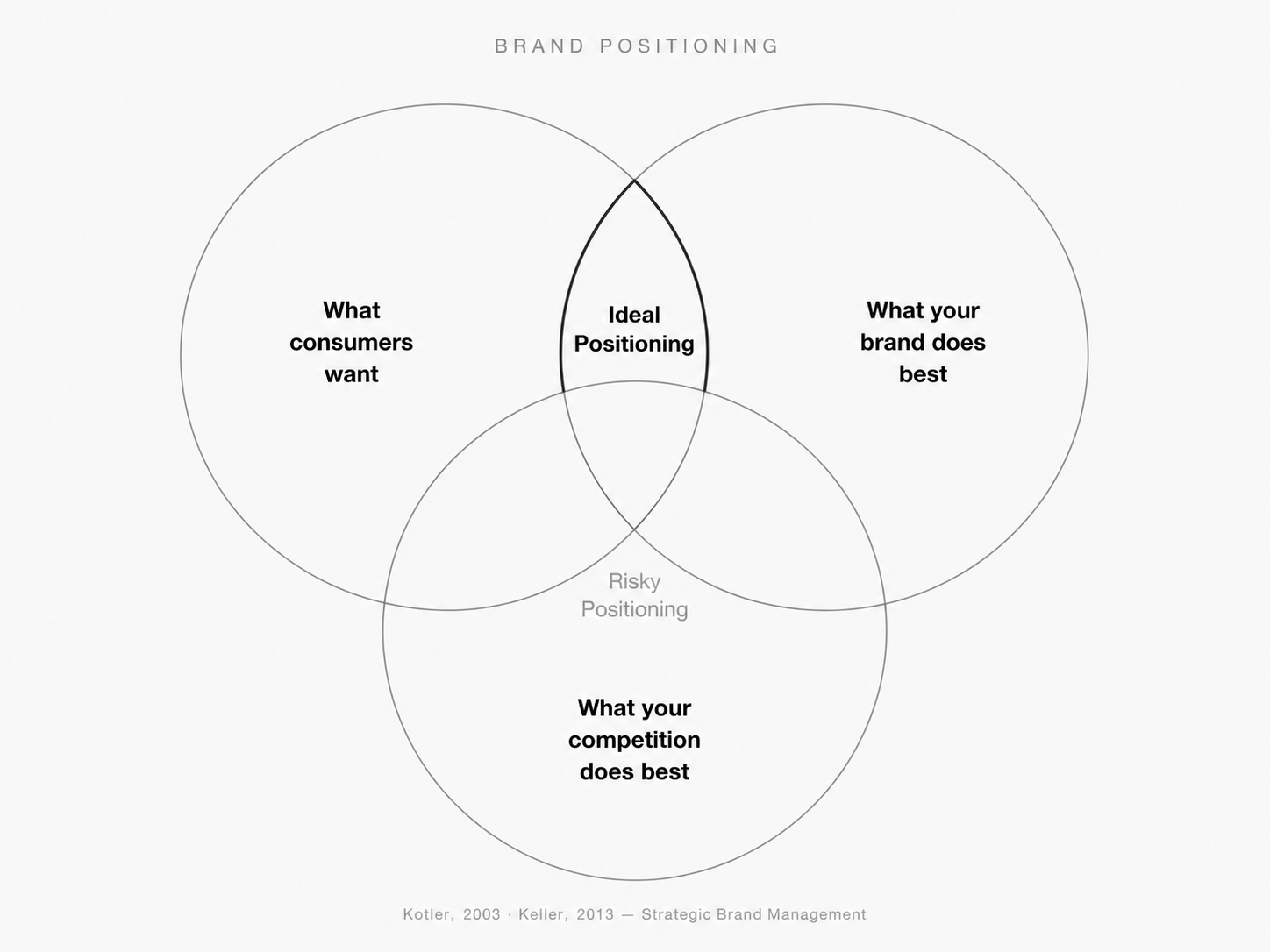
Ideal brand positioning. Brand positioning requires three analyses: what the target patient values, what the practice can genuinely deliver, and what competitors already occupy. Where all three conditions are met, a viable position exists. Everything that follows, including the brand’s visual identity and communication tone, is an expression of it.
Positioning requires choice. When a brand tries to occupy conflicting positions, the result is often ambiguity. The strongest practices rarely try to appeal to every patient. Instead, they define which patients they seek to serve best, and build their brand around that audience. A practice without a clearly defined position may appeal to patients with a broad range of expectations and aesthetic preferences, whereas a clearly positioned practice is more likely to attract patients whose expectations already align with its approach.
People respond more favorably to brands whose image aligns with how they see or would like to see themselves, or how they want to be perceived by others. Related research on self-brand connections shows that consumers can use brands to construct and express self-concept. Careful research of the preferences of the target patient segment helps make choices that communicate preferences that feel congruent with the patient’s values.
Operationally, a defined position gives the practice a shared standard for daily decisions. What is posted on Instagram? How does the consultation room feel? What kind of web design supports the practice’s goals the best? How are patient inquiries handled? Without brand positioning, these decisions depend on individual instinct. With one, they accumulate into a more consistent patient experience.
The Commercial Value of a Distinct Reputation
The advantages of clear brand positioning extend beyond the immediate patient relationship. A defined position can also create commercial value and media access that extends beyond the surgeon’s personal reputation.
Price sensitivity is highest when a patient perceives options as equivalent. When practices occupy the same undifferentiated space, the decision is made on secondary factors: who quoted the lowest, who is closest, who responded first. Therefore, a positioned practice is better protected from competitive pressure. When a new surgeon enters the market with lower fees, newer technology, or a larger social media following, an unpositioned practice is more exposed because patients may compare it on those same terms. A positioned practice has a stronger buffer because patients choose it for a specific meaning, standard, aesthetic perspective, or experience that competitors cannot instantly copy.
The further advantage is media recognition. A surgeon with a defined, articulable position can be pitched in a single sentence to a media representative. A surgeon who is excellent but undefined is harder to describe, regardless of the quality of their outcomes. Press coverage, editorial features, and platform visibility tend to concentrate around practitioners who have given others a clear reason to talk about them.
A practice with a strong brand position is worth more as a business than one without it, even when the clinical quality is comparable. If the surgeon steps back, brings in a partner, or eventually sells, personal reputation can be difficult to transfer cleanly. Brand equity, meaning the accumulated associations, patient expectations, and market position a defined brand holds, can be more transferable than personal reputation alone.
Related research highlights how patient experience shapes trust and loyalty in medical-aesthetic services. The physical environment of the clinic and the way staff present themselves can contribute to patient satisfaction and long-term loyalty. These findings suggest that patients’ perceptions of professionalism and care quality extend beyond medical outcomes and are shaped by the overall experience of the clinic.
About the Author
Jen Ahlsten is the founder of Vitruviani and author of Eminence: The New Standard for Plastic Surgery Marketing. She studies the disconnect between the standard of care surgeons deliver and the way their practices are presented online to prospective patients.
Sources
Ahlsten, J. (2025). Branding in aesthetic plastic surgery: Patient perception of branded vs. unbranded practices. Exploratory perception study. ResearchGate.
Ahlsten, J. (2026). Eminence: The New Standard for Plastic Surgery Marketing. Vitruviani.
Bank, J., Feingold, R. S., Korn, P., Light, D., & Israeli, R. (2023). Branding a plastic surgery group practice: A case study. Plastic and Reconstructive Surgery.
Brandão, A., & Ribeiro, L. (2023). The impact of patient experience on loyalty in the context of medical-aesthetic health services. SAGE Open Medicine.
Damasio, A. R. (1994). Descartes' error: Emotion, reason, and the human brain. Putnam.
Escalas, J. E., & Bettman, J. R. (2003). You are what they eat: The influence of reference groups on consumers' connections to brands. Journal of Consumer Psychology, 13(3).
Kahneman, D. (2011). Thinking, fast and slow. Farrar, Straus and Giroux.
Keller, K. L. (1993). Conceptualizing, measuring, and managing customer-based brand equity. Journal of Marketing, 57(1).